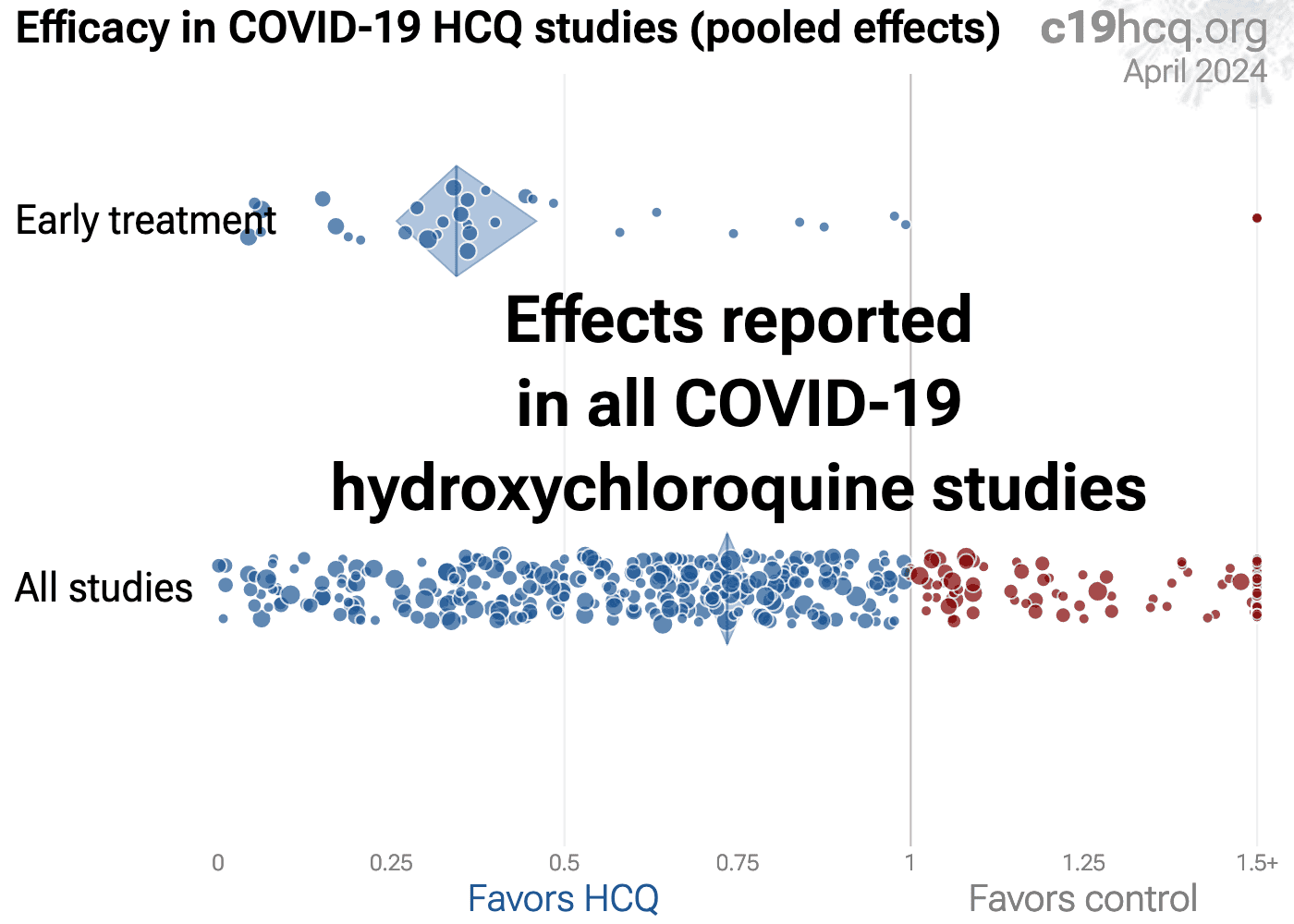
Early treatment shows 66% [54‑74%] lower risk with pooled effects in 39 studies. Results are similar for higher quality studies and for peer-reviewed studies. The 17 mortality and 16 hospitalization results show 76% [61‑85%] lower mortality and 41% [28‑51%] lower hospitalization.
Late treatment is less successful, with 20% [16‑24%] lower risk from 269 studies. Very late treatment may be harmful, especially with excessive dosages.
Randomized Controlled Trials show 19% [6‑30%] lower risk, or 25% [11‑37%] when excluding late treatment.
There is substantial bias towards publishing negative results. Prospective studies show higher efficacy. Negative RCTs received priority treatment at top journals, while positive trials report difficulty publishing. There is a strong geographical bias, with significantly more negative studies from North America.
Results are missing for 53% of early treatment and prophylaxis RCTs, compared to 18% for late treatment, consistent with the higher prevalence of positive studies for early treatment and prophylaxis, and bias against publishing positive results.
No treatment or intervention is 100% effective. All practical, effective, and safe means should be used based on risk/benefit analysis. Multiple treatments are typically used in combination, which may be significantly more effective. Lung pharmacokinetics show high inter-individual variability Ruiz.
All data to reproduce this paper and the sources are in the appendix. Multiple other meta analyses show efficacy for early treatment or prophylaxis García-Albéniz, Ladapo, Landsteiner de Sampaio Amêndola, Prodromos, Risch, Risch (B), Stricker.

{kind=link}