This meta analysis is designed to exclude most studies. Authors
select a small subset of studies, with a majority of results based on only 1
or 2 studies. Authors split up studies which dilutes the effects and results
in a lack of statistical significance for most outcomes. Authors perform 16+
meta analyses with very few studies in each analysis, and do not combine the
evidence from all studies. However, we can consider the probability of the
observed results across all outcomes.
Authors find positive results for 11 of 12 primary efficacy
outcomes with events, or 16 of 18 including secondary outcomes. One of the
primary outcomes and two of the secondary outcomes show statistically
significant improvements in isolation. If we assume independence, the
probability that 11+ of 12 primary efficacy outcomes were positive for an
ineffective treatment is p = 0.003. For 16+ of 18 outcomes we get
p = 0.0007. This simple analysis does not take into account the
magnitude of positive effects, or the dependence due to some studies
contributing multiple outcomes, however observation suggests that a full
analysis of the combined evidence is likely to show efficacy.
The study is entirely retrospective in the current version. The
protocol is dated April 20, 2021, and the most recent study included is from
March 9, 2021. The protocol was modified after publication in order to include
a close to null result (
Beltran Gonzalez "patients discharged without
respiratory deterioration or death at 28 days"), so the current protocol is
dated July 28, 2021.
Authors excluded many studies by requiring results at a
specific time, for example mortality, ventilation, etc. required results at
exactly 28 days. Authors excluded all prophylaxis studies by requiring
results at exactly 14 days.
Studies comparing with other medications were excluded, however
these studies confirm efficacy of ivermectin. The only case where they could
overstate the efficacy of ivermectin is if the other medication was harmful.
There is some evidence of this for excessive dosage/very late stage use,
however that does not apply to any of the studies here.
Studies using combined treatment were excluded, even when it is
known that the other components have minimal or no effect. 3 of 4 RCTs with
combined treatment use doxycycline in addition, which was shown to have no
significant effect in
Butler. Other studies were excluded by
requiring PCR confirmation.
Authors are inconsistent regarding active comparators. They
state that hydroxychloroquine “does not work”, yet excluded trials comparing
ivermectin to a drug they hold to be inactive. On the other hand, remdesivir
was an acceptable comparator, although it is considered to be effective
standard of care in some locations
Fordham.
Authors fail to recognize that Risk of Bias (RoB) domains such
as blinding are far less important for the objective outcome of
mortality.
Authors include
Beltran Gonzalez as "moderate"
COVID-19, however patients in this study were in severe condition (baseline
SatO2 83).
Fordham summarizes several problems:
•unsupported assertions of adverse
reactions to ivermectin, and the outdated claim that unsafe dosing would be
needed to be effective;
•a demand for PCR or antigen testing,
without analysis of reliability and not universally available even in
developed countries at the start of the pandemic;
•contradictions in the exclusion
criteria, including placebo and approved SoC comparators, but rejecting
hydroxychloroquine, though held to be ineffective (and an approved SoC in
some jurisdictions);
•inclusion of “deemed active”
comparators whilst excluding “potentially active” ones;
•exclusion of combination therapies,
though the norm among practising clinicians;
•the rejection of other than RCTs when
the objective is a “complete evidence profile”;
•arbitrary time-points for outcome
measures, excluding non-compliant trials;
•fragmentation of data by location of
care under varying hospitalisation criteria;
•the resulting focus on a small
fraction of the available clinical evidence, with most comparisons based on
single studies with no meta-analysis possible;
•a resulting inpatient mortality
comparison with fewer patients than a June 2020 confounder-matched
study;
•no conclusion on the headline
mortality outcome, when multiple lines of evidence from elsewhere
(including the WHO) point to significant mortality advantage.
Cochrane was reputable in the past, but is now controlled by
pharmaceutical interests. For example, see the news related to the expulsion
of founder Dr. Gøtzsche and the associated mass resignation of board members
in protest
blogs.bmj.com, bmj.com, en.x-mol.com.
For another example of bias see
ebm.bmj.com.
The BiRD group gave the following early comment: "Yesterday’s
Cochrane review surprisingly doesn’t take a pragmatic approach comparing
ivermectin versus no ivermectin, like in the majority of other existing
reviews. It uses a granular approach similar to WHO’s and the flawed Roman et
al paper, splitting studies up and thereby diluting effects. Consequently,
the uncertain conclusions add nothing to the evidence base. A further
obfuscation of the evidence on ivermectin and an example of research waste.
Funding conflicts of interests of the authors and of the journal concerned
should be examined."
For dicussion of issues added in the updated version see
Popp.
Authors report funding from the German Federal Ministry of
Education and Research, which may be influenced by
gcgh.grandchallenges.org.
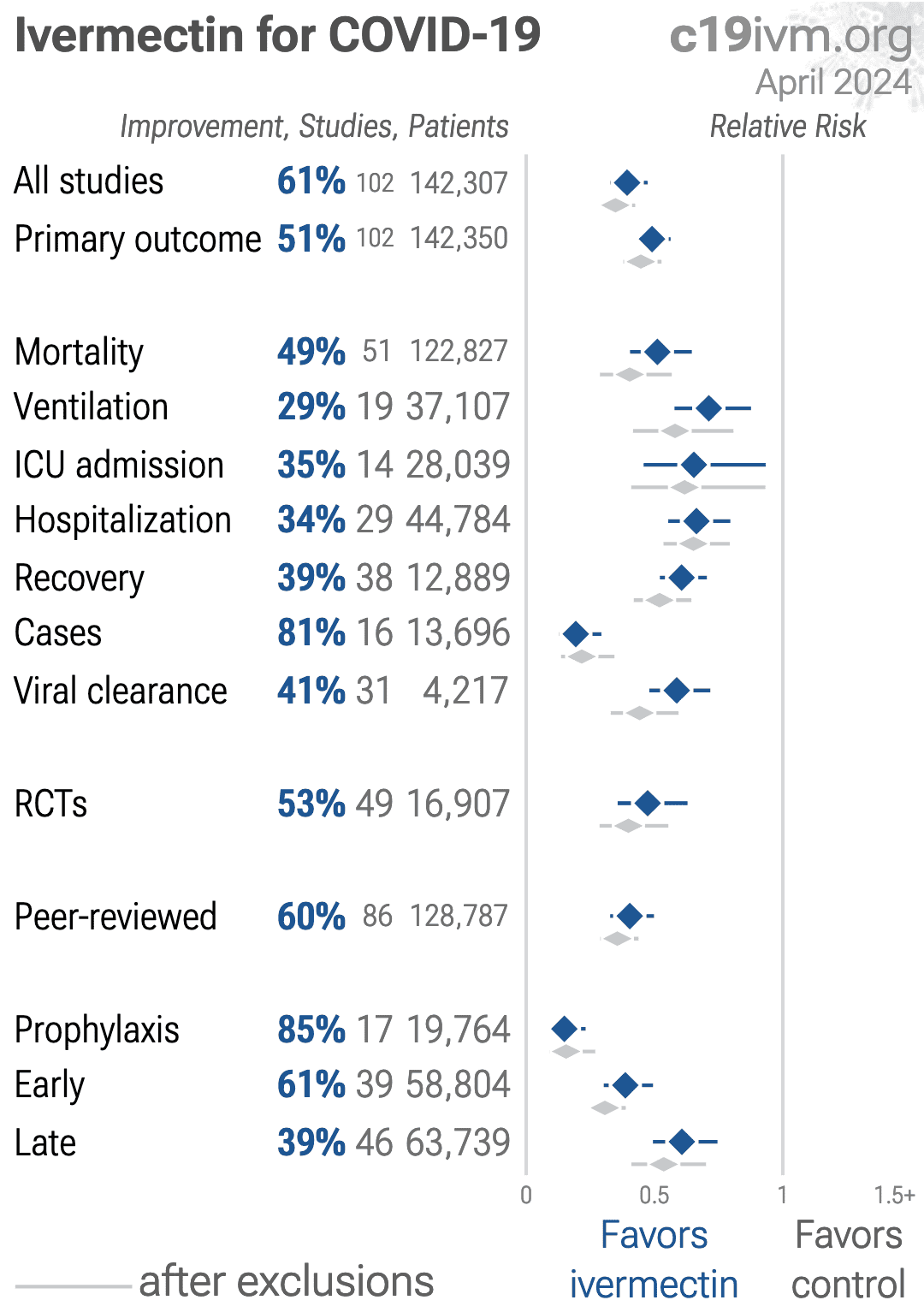
Currently there are
102 ivermectin for COVID-19 studies, showing 49% lower mortality
[35‑60%], 29% lower ventilation
[12‑42%], 35% lower ICU admission
[7‑54%], 34% lower hospitalization
[20‑45%], and 81% fewer cases
[71‑87%].
Popp et al., 28 Jul 2021, preprint, 8 authors.
Ivermectin for preventing and treating COVID-19
Maria Popp, Miriam Stegemann, Maria-Inti Metzendorf, Susan Gould, Peter Kranke, Patrick Meybohm, Nicole Skoetz, Stephanie Weibel
Cochrane Database of Systematic Reviews, doi:10.1002/14651858.cd015017.pub2
Analysis 1.2. Comparison 1: Ivermectin compared to placebo or standard of care for people with moderate-to-severe COVID-19 treated in the inpatient setting, Outcome 2: Worsening of clinical status -need for invasive mechanical ventilation up to 28 days (primary analysis
CONSORT 2010 Statement Schulz KF, Altman DG, Moher D, for the CONSORT Group. CONSORT 2010 Statement: updated guidelines for reporting parallel group randomised trials. BMC Medicine 2010;8:18.
COVID Guidelines India 2021 Covid Management Guidelines India Group. COVID Management Guidelines India. indiacovidguidelines.org/ivermectin/ (accessed 15 May 2021).
COVID-NMA Working Group COVID-NMA working group. The COVID-NMA initiative: a living mapping and living systematic review of Covid-19 trials. covidnma.com (accessed prior to 1 July 2021).
Cochrane
Library Trusted evidence. Informed decisions. Better health.
Supplementary File_Ivermectin_Risk of Bias Weibel S, Popp M. Supplementary File_Ivermectin_Risk of Bias Excel Tool (Version 1). Zenodo 2021. • Inclusion criteria: aged 18-65 years; admitted to hospital within last 7 days; presence of fever (37.5 °C), cough, sore throat, or a combination; diagnosed positive for SARS-CoV-2 by rRT-PCR • Exclusion criteria: allergic to ivermectin or doxycycline, or if here was the potential for a drug-drug interaction with ivermectin or doxycycline; had chronic illnesses (e.g. ischaemic heart disease, heart failure, documented cardiomyopathy, chronic kidney disease, chronic liver disease); had received ivermectin or doxycycline (or both) in the last 7 days; were pregnant or lactating; or had participated in any other clinical trial within last month Interventions
Cochrane Database of Systematic Reviews
Study characteristics
..
References
Deeks, Higgins, Altman, Chapter 10: Analysing data and undertaking meta-analyses
Garegnani, Madrid, Meza, Misleading clinical evidence and systematic reviews on ivermectin for COVID-19, BMJ Evidence Based Medicine
German Awmf Guideline, None
Goetz, Magar, Dornfeld, Giese, Pohlmann et al., Influenza A viruses escape from MxA restriction at the expense of e icient nuclear vRNP import, Scientific Reports,
doi:10.1038/srep23138González-Canga, None
González-Canga, Sahagún-Prieto, Diez-Liébana, Fernández-Martínez, Vega et al., The pharmacokinetics and interactions of ivermectin in humans, Journal of the American Association of Pharmaceutical Scientists,
doi:10.1208/s12248-007-9000-9]Herrmann2020Herrmann, Adam, Notz, Helmer, Sonntagbauer et al., COVID-19 induced acute respiratory distress syndrome -a multicenter observational study
Higgins, Lasserson, Chandler, Tovey, Thomas et al., Methodological Expectations of Cochrane Intervention Reviews
Hill, Abdulamir, Ahmed, Ashgar, Babalola et al., Meta-analysis of randomized trials of ivermectin to treat SARS-CoV-2 infection,
doi:10.21203/rs.3.rs-148845/v1Ivmmeta, com Ivermectin for COVID-19: real-time meta analysis of 60 studies
Karagiannidis, Mostert, Hentschker, Voshaar, Malzahn et al., Case characteristics, resource use, and outcomes of 10 021 patients with COVID-19 admitted to 920 German hospitals: an observational study, Lancet Respiratory Medicine,
doi:10.1016/S2213-2600(20)30316-7Kluge, Janssens, Welte, Weber-Carstens, Schälte et al., S3-Guideline -recommendations on Inpatient Treatment of Patients With COVID-19
Kobayashi, Jung, Linton, Kinoshita, Hayashi et al., Communicating the risk of death from novel coronavirus disease (COVID-19), Journal of Clinical Medicine,
doi:10.3390/jcm9020580Panahi, Poursaleh, Goldust, The e icacy of topical and oral ivermectin in the treatment of human scabies, Annals of Parasitology
Prescott, Girard, RECOVERY 2021 Recovery Collaborative Group. Dexamethasone in hospitalized patients with Covid-19, New England Journal of Medicine,
doi:10.1001/jama.2020.14103Rodríguez-Mega, None
Schünemann, Higgins, Vist, Glasziou, Akl et al., Chapter 14: Completing 'Summary of findings' tables and grading the certainty of the evidence
Siemieniuk, Rochwerg, Agoritsas, Lamontagne, Leo et al., A living WHO guideline on drugs for Covid-19, BMJ,
doi:10.1136/bmj.m3379Singh, Ryan, Kredo, Chaplin, Fletcher, Chloroquine or hydroxychloroquine for prevention and treatment of COVID-19, Cochrane Database of Systematic Reviews,
doi:10.1002/14651858.CD013587.pub2Sterne, Savović, Page, Elbers, Blencowe et al., RoB 2: a revised tool for assessing risk of bias in randomised trials, BMJ,
doi:10.1136/bmj.l4898


{kind=link}