REGEN-COV Antibody Combination and Outcomes in Outpatients with Covid-19
David M Weinreich, Sumathi Sivapalasingam, Thomas Norton, Shazia Ali, Haitao Gao, Rafia Bhore, Jing Xiao, Andrea T Hooper, Jennifer D Hamilton, Bret J Musser, Diana Rofail, Mohamed Hussein, Joseph Im, Dominique Y Atmodjo, Christina Perry, Cynthia Pan, Adnan Mahmood, Romana Hosain, John D Davis, Kenneth C Turner, Alina Baum, Christos A Kyratsous, Yunji Kim, Amanda Cook, Wendy Kampman, Lilia Roque-Guerrero, Gerard Acloque, Hessam Aazami, Kevin Cannon, J Abraham Simón-Campos, Joseph A Bocchini, Bari Kowal, A Thomas Dicioccio, Yuhwen Soo, Gregory P Geba, Neil Stahl, Leah Lipsich, Ned Braunstein, Gary Herman, George D Yancopoulos
New England Journal of Medicine, doi:10.1056/nejmoa2108163
BACKGROUND In the phase 1-2 portion of an adaptive trial, REGEN-COV, a combination of the monoclonal antibodies casirivimab and imdevimab, reduced the viral load and number of medical visits in patients with coronavirus disease 2019 (Covid-19). REGEN-COV has activity in vitro against current severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) variants of concern.
METHODS In the phase 3 portion of an adaptive trial, we randomly assigned outpatients with Covid-19 and risk factors for severe disease to receive various doses of intravenous REGEN-COV or placebo. Patients were followed through day 29. A prespecified hierarchical analysis was used to assess the end points of hospitalization or death and the time to resolution of symptoms. Safety was also evaluated.
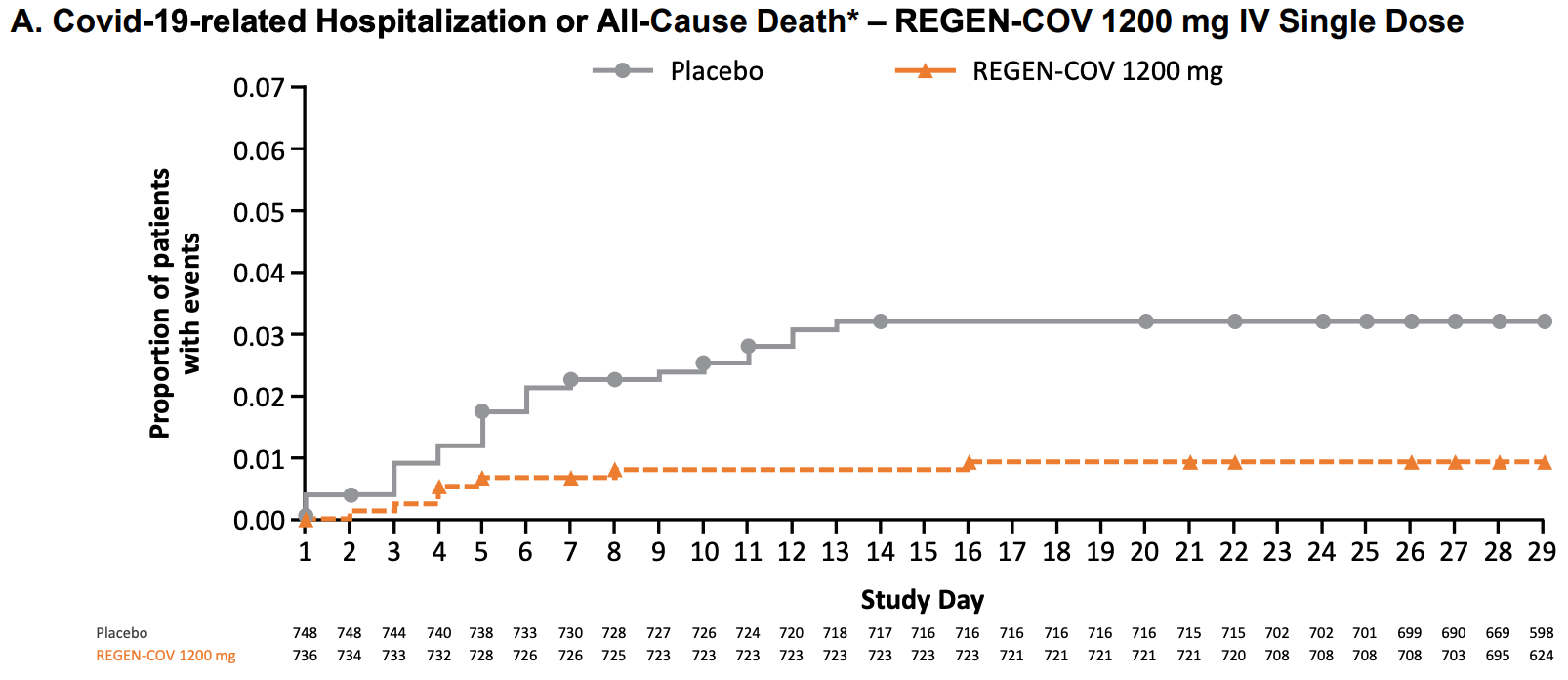
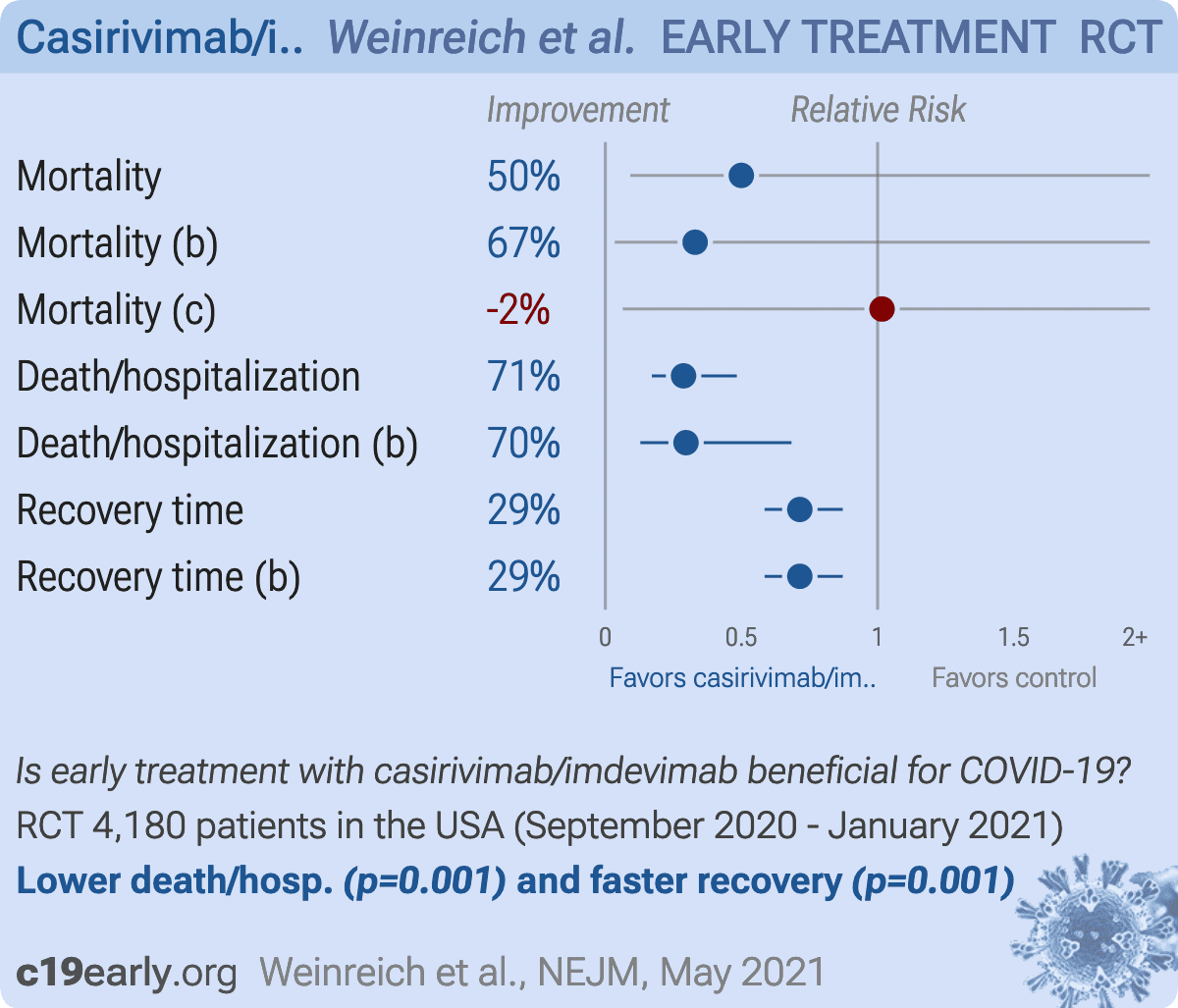
RESULTS Covid-19-related hospitalization or death from any cause occurred in 18 of 1355 patients in the REGEN-COV 2400-mg group (1.3%) and in 62 of 1341 patients in the placebo group who underwent randomization concurrently (4.6%) (relative risk reduction [1 minus the relative risk], 71.3%; P<0.001); these outcomes occurred in 7 of 736 patients in the REGEN-COV 1200-mg group (1.0%) and in 24 of 748 patients in the placebo group who underwent randomization concurrently (3.2%) (relative risk reduction, 70.4%; P = 0.002). The median time to resolution of symptoms was 4 days shorter with each REGEN-COV dose than with placebo (10 days vs. 14 days; P<0.001 for both comparisons). REGEN-COV was efficacious across various subgroups, including patients who were SARS-CoV-2 serum antibody-positive at baseline. Both REGEN-COV doses reduced viral load faster than placebo; the least-squares mean difference in viral load from baseline through day 7 was −0.71 log 10 copies per milliliter (95% confidence interval [CI], −0.90 to −0.53) in the 1200-mg group and −0.86 log 10 copies per milliliter (95% CI, −1.00 to −0.72) in the 2400-mg group. Serious adverse events occurred more frequently in the placebo group (4.0%) than in the 1200-mg group (1.1%) and the 2400-mg group (1.3%); infusion-related reactions of grade 2 or higher occurred in less than 0.3% of the patients in all groups.
CONCLUSIONS REGEN-COV reduced the risk of Covid-19-related hospitalization or death from any cause, and it resolved symptoms and reduced the SARS-CoV-2 viral load more rapidly than placebo. (Funded by Regeneron Pharmaceuticals and others; ClinicalTrials .gov number, NCT04425629.
Disclosure forms provided by the authors are available with the full text of this article at NEJM.org. A data sharing statement provided by the authors is available with the full text of this article at NEJM.org. We thank the trial participants; their families; the investigational site members involved in this trial (principal and subprincipal investigators, listed in the Supplementary Appendix); the Regeneron trial team (members listed in the Supplementary Appendix); the members of the independent data and safety monitoring committee; Brian Head, Ph.D., Caryn Trbovic, Ph.D., and S. Balachandra Dass, Ph.D., of Regeneron Pharmaceuticals for assistance with development of an earlier version of the manuscript; and Prime for assistance with the formatting and copy editing of an earlier version of the manuscript.
Appendix The authors' full names and academic degrees are as follows: David M. Weinreich
References
Baum, Ajithdoss, Copin, REGN-COV2 antibodies prevent and treat SARS-CoV-2 infection in rhesus macaques and hamsters, Science
Baum, Fulton, Wloga, Antibody cocktail to SARS-CoV-2 spike protein prevents rapid mutational escape seen with individual antibodies, Science
Challen, Brooks-Pollock, Read, Dyson, Tsaneva-Atanasova et al., Risk of mortality in patients infected with SARS-CoV-2 variant of concern 202012/1: matched cohort study, BMJ
Copin, Baum, Wloga, The monoclonal antibody combination REGEN-COV protects against SARS-CoV-2 mutational escape in preclinical and human studies, Cell
Davies, Abbott, Barnard, Estimated transmissibility and impact of SARS-CoV-2 lineage B.1.1.7 in England, Science
Del Rio, Collins, Malani, Longterm health consequences of COVID-19, JAMA
Farrington, Manning, Test statistics and sample size formulae for comparative binomial trials with null hypothesis of non-zero risk difference or non-unity relative risk, Stat Med
Hansen, Baum, Pascal, Studies in humanized mice and convalescent humans yield a SARS-CoV-2 antibody cocktail, Science
Logue, Franko, Mcculloch, Sequelae in adults at 6 months after COVID-19 infection, JAMA Netw Open
Nalbandian, Sehgal, Gupta, Post-acute COVID-19 syndrome, Nat Med
Onder, Rezza, Brusaferro, Casefatality rate and characteristics of patients dying in relation to COVID-19 in Italy, JAMA
Rofail, Mcgale, Im, Development and content validation of the Symptoms Evolution of COVID-19: a patient-reported electronic daily diary in clinical and real-world studies,
doi:10.1101/2021.07.06.21259654v1Stokes, Zambrano, Anderson, Coronavirus disease 2019 case surveillance -United States, January 22, MMWR Morb Mortal Wkly Rep
Wang, Nair, Liu, Antibody resistance of SARS-CoV-2 variants B.1.351 and B.1.1.7, Nature
Weinreich, Sivapalasingam, Norton, REGN-COV2, a neutralizing antibody cocktail, in outpatients with Covid-19, N Engl J Med
Williamson, Walker, Bhaskaran, Factors associated with COVID-19-related death using OpenSAFELY, Nature
Wu, Mcgoogan, Characteristics of and important lessons from the Coronavirus Disease 2019 (COVID-19) outbreak in China: summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention, JAMA
Xie, Liu, Liu, Neutralization of SARS-CoV-2 spike 69/70 deletion, E484K and N501Y variants by BNT162b2 vaccineelicited sera, Nat Med


{kind=link}
{kind=link}